
Original in Russian is available at the link: С.В. Архипова «Почему восстановление вертлужной губы может быть неэффективно?» (06.04.2025), below is a machine translation edited by a non-native speaker (version dated 06/04/2025).
Abstract
Acetabular
labrum repair and reconstruction do not prevent hip joint instability during
gait and the development of osteoarthritis in the case of an elongated
ligamentum capitis femoris. This conclusion is based on mathematical
calculations and analysis of experiments conducted on a mechanical hip joint
model.
Keywords: arthroscopy, hip joint, acetabular labrum, ligamentum capitis femoris,
ligamentum teres, ligament of head of femur, reconstruction, repair
Introduction
Nearly 80%
of primary hip arthroscopies involve labral repair (2019WestermannRW_RosneckJT).
Reconstruction is the most common procedure for addressing labral pathology and
during revision arthroscopy (2020MaldonadoDR_DombBG). Numerous support groups
on Facebook exist for individuals who have undergone such treatments. Unfortunately,
patient feedback is not always positive.
A cause of
poor outcomes after labral surgery may lie in changes to the ligamentum capitis
femoris (LCF). This strong internal ligament is an important stabilizer of the
hip joint (2012CerezalL_Pérez-CarroL). However,
as early as 1833, P.N. Gerdy, based on morphological studies, stated that the
LCF could contribute to hip dislocation. We have verified and refined the
opinion of the authoritative anatomist through experiments on a mechanical
model of the hip joint.
It was found that tension of the LCF, with normal length and attachment locations, presses the acetabulum against the femoral head (2024aАрхиповСВ). Conversely, tension of an elongated LCF with peripherally displaced proximal attachment separates the acetabulum from the femoral head, provoking subluxation (2024bАрхиповСВ). This is due to a radical change in the direction of the horizontal force generated by the elongated LCF (Fig. 1).
 |
| Figure 1. Direction of horizontal force (Fhor) with normal (top) and elongated (bottom) LCF; left – mechanical model experiments, right – schematic diagrams (author’s illustrations). |
The Hip
Joint’s "Dark Matter"
It is
widely accepted that during single-leg stance, the abductor muscle group
prevents the pelvis, tilted downwards, from falling in the medial direction (1993BombelliR;
2012PauwelsF). A key role is played by the horizontal component of muscular
effort, which presses the acetabulum against the femoral head (Fig. 2).
However,
according to A.I. Kapandji (2009), the primary
abductor muscles collectively generate a force (Fabd) equivalent to 28.5 kg
(gluteus medius – 16 kg; gluteus minimus – 4.9 kg; tensor fasciae latae – 7.6
kg). If positioned at a 60º angle to the horizontal, their combined tension
would produce a horizontal force (Fhor) of 14.25 kg,
calculated as:
Fhor = Fabd × cos60º (1).
 |
| Figure 2. Diagram illustrating the compression effect of the acetabulum on the femoral head in a single-leg stance; Fhor – horizontal force, Fabd – abductor muscle group effort (adapted from 1965StrangeFGStC, with our additions). |
Additional
compression of the femoral head against the acetabulum arises from negative
pressure during attempts to separate the joint. This is provided by the
continuity of the acetabular synovial membrane, synovial fluid, and the labrum.
Normally, this suction seal is equivalent to about 100 pounds or 45.36 kg (2025MortensenAJ_AokiSK).
Thus, the muscles and labrum together generate a force equivalent to an average
traction of 59.61 kg.
Assuming
body mass of 58.7 kg, during single-leg stance, the mass to stabilize over the
hip joint is 47.76 kg (2012PauwelsF). This suggests that the abductor muscles
and labrum can counteract forces separating the femoral head and acetabulum
when the pelvis tilts downward.
During
walking, inertial forces act on body segments. The maximum dynamic force,
equivalent to 24.35 kg, occurs in the 17th phase of the gait cycle (2012PauwelsF). Therefore, during the mid-stance phase of the gait cycle (single-leg stance),
the separating load can reach 72.11 kg.
 |
| Figure 3. Pelvic tilt toward the non-supporting side (the norm) during single-leg stance – 4º (left), and mid-stance phase of the gait cycle – 3º (right) (from 2012АрхиповСВ, with additions). |
In a healthy individual standing on one leg and mid-stance phase of the
gait cycle, the pelvis tilts downward (Fig. 3). Common sense and our
calculations suggest that dislocation should occur during walking. An additional
force of at least 12.5 kg is needed to reinforce the joint. Thus, we conclude
that labral repair (reconstruction) ensures hip stability in a single-leg
stance but not during walking. This implies the existence of an anatomical
structure or effect generating the missing force.
Normal-Length
LCF
Our
experiments with the mechanical model revealed the presence of a lateral force,
which, among other things, prevents dislocation when standing on one leg. This
is generated by the tension of LCF oriented upward and outward. This structure
resembles the mysterious "dark matter" of cosmology (2022Chadha-DayF_MarshDJ).
Opinions on it, as well as on the LCF, are conflicting. The function of the LCF
in the natural joint remains poorly understood and debated. The role of the LCF
is primarily assessed through anatomical specimens, models, calculations, and
reasoning.
Under the
weight of a body supported on one leg, the LCF tenses, generating a reaction
force (Fr), or elastic force, equal in magnitude to the
acting body weight (m) if vertically aligned, and decreasing with
deviation:
Fr = mg
× cosα (2).
For a body
mass of 47.76 kg at rest and an LCF angled 20º from the vertical, the reaction
force is 440.27 N. The horizontal component (Fhor) is
calculated as:
Fhor = Fr
× sin20º (3).
Directed
laterally (Fig. 1a), it equals 150.57 N, or 15.35 kg. Combined with muscle
contraction and the labrum’s effect of suction seal, this increases the
potential compressive force in the hip join to 74.96 kg during single-leg
stance.
During
walking, centrifugal force (Fc) further affects the LCF. It depends on the
speed of movement (v), the acting mass of the body (m) and the length of the
LCF (L):
Fc = mg × v2 / Llcf (4).
With
parameters of 47.76 kg, LCF length of 0.025 m, which moves at a speed of 0.04
m/s, centrifugal force equals 29.98 N, or approximately 3.05 kg. Thus, in the
mid-stance phase of the gait cycle, with the LCF at a 20º angle (open downward
and medially), the reaction force reaches 470.25 N, with a lateral horizontal
component of 160.82 N, or 16.39 kg (Eq. 3). In a healthy individual, the tensed
LCF, muscles, and labrum can resist a joint-separating traction of 76.00 kg,
explaining why a 72.11 kg load during walking does not cause dislocation with a
normal LCF.
LCF reaction force is directed upward, countering body weight that reducing pressure on the femoral head. This is supported by mechanical model experiments (2024cАрхиповСВ) and a simplified equation for pelvic equilibrium in the frontal plane during single-leg stance:
0 = mgL + FabdL1 - FrL2 (5),
where L is the lever arm of body weight (mg),
L1
is the lever arm of the abductor muscle group (Fabd), and L2 is the LCF reaction force arm (Fr).
Our
experiments showed that the acetabular labrum has minimal influence on
torsional moments in the frontal plane (2024dАрхиповСВ, Fig. 4). Its retaining function is more relevant to
translational motion of the femoral head. The stabilizing role of the
acetabular labrum is greatest in preventing the outward (laterally downward)
translational movement of the femoral head with a fixed pelvis, or inward
acetabular displacement (medially upward) with a fixed femur.
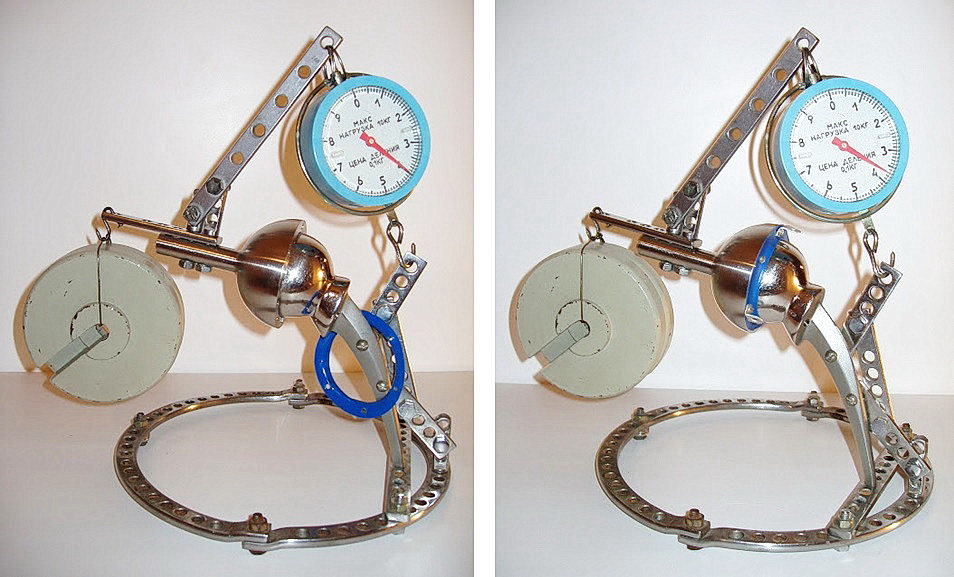 |
| Figure 4. Experiments on a mechanical model: changing of the abductor muscle analog effort in the absence of an acetabular labrum analogue (left) and the presence of an acetabular labrum analogue (right); a 2 kg load is suspended from the acetabulum model (photos by the author). |
Elongated LCF
In mechanical model experiments, elongation of the LCF was simulated by
shifting the proximal attachment outward (2024bАрхиповСВ). In the real hip joint, this corresponds to a partial
avulsion of the proximal end of the LCF. Post-transformation of our mechanical
model, the LCF analog adopted an opposite orientation, with its axis tilted
upward and inward. Tension of the LCF in this position caused medial displacement
of the acetabular model (Fig. 1b).
For a tensioned LCF inclined at 20º (angle open downwards and
laterally), in a single-leg stance with a 47.76 kg mass, the reaction force
reaches 440.27 N (Eq. 2). Its horizontal component (Fhor), directed medially, is 150.57 N, or 15.35 kg (Eq. 3).
This force tends to displace the acetabulum off the femoral head. In a
natural hip joint, there will be a tendency to dislocation. It is prevented by:
the abductor muscle group and the acetabular labrum, which provides a suction
seal. The listed structures are normally effective with an average traction of
59.61 kg. At the same time, the horizontal component of the reaction force of
the tensioned LCF will reduce the threshold of resistance to dislocation to
44.26 kg. The obtained value is less than the effective body weight in a
single-support pose of 47.76 kg (2012PauwelsF).
Where the pelvis is tilted medially, this condition results in
subluxation, which inevitably stretches the joint capsule and external
ligaments, causing discomfort or pain. Relief is achieved by tilting the pelvis
upward and laterally. Arthroscopic evidence confirms that in early hip
osteoarthritis, the LCF is often damaged, dystrophically altered, or absent (1998ByrdJW;
2001МалаховаСО; 2004ОрлецкийАК_ОгаревЕВ; 2006RuhmannO_BohnsackM).
Patients with LCF pathology intuitively raise the pelvis, lean their
torso, or extend an arm toward the affected side during single-leg stance or
mid-stance phase of the gait cycle. Our data show that in individuals without
hip pathology, pelvic tilt downward in single-leg stance is 5.8±2.4º; in stage
1 coxarthrosis, it is 2.3±1.9º; and in stages 2-3, it tilts upward by 4.6±2.5º.
Of the 82 examined individuals with osteoarthritis of the hip joint, 78 had a
pelvic tilt to the non-supporting side in the mid-stance phase of the step that
was less than the norm of 2.2±1.7°. Excessive arm abduction and its imbalance
were observed in 79 cases, with spinal deviation toward the supporting side
averaging 7.1±3.1º (vs. 1.9±2.0º normal) across all coxarthrosis stages (2012,2023АрхиповСВ).
Lateral
pelvic tilt eliminates subluxation risk, including by relaxing the LCF.
However, compensatory disruption of posture and gait has detrimental effects on
the musculoskeletal system. Without an adequately functioning LCF, which is an
additional flexible support for the body, the average daily pressure on the
upper segment of the femoral head increases (Eq. 5). In adults, this provokes:
subluxation, formation of intraosseous cysts, abrasion of cartilage or
so-called "aseptic necrosis" of the femoral head, which always end in
osteoarthritis (Fig. 5).
 |
| Figure 5. Femoral head removed during hip replacement for osteoarthritis, with cartilage wear zone indicated (from 2012АрхиповСВ , with additions). |
In our
view, elongated LCF in children may, beyond subluxation, lead to coxa magna or
Legg-Calvé-Perthes disease.
Conclusion
Calculations
highlight the LCF’s critical role in hip joint stabilization. Partial proximal
detachment LCF with elongation promote subluxation during single-leg stance. To
solve this problem, restoration of the normal length of the LCF and proximal
attachment is required. Without this, surgical treatment of the acetabular
labrum injury is ineffective, since isolated labral repair does not prevent
instability during walking and osteoarthritis.
References
Bombelli R. Structure and function in normal and abnormal hip: how to rescue mechanically jeopardized hip. 3-rd. ed., rev. and enl. p. Berlin, Heidelberg, New York: Springer Verlag, 1993. link.springer.com
Byrd JW. Operative hip arthroscopy. New York: Thieme, 1998. chamblinbookmine.com
Cerezal L, Arnaiz J, Canga A, Piedra T, Altónaga JR, Munafo R, Pérez-Carro L. Emerging topics on the hip: ligamentum teres and hip microinstability. European journal of radiology. 2012;81(12)3745-54. artroscopiaycadera.es
Chadha-Day F, Ellis J, Marsh DJ. Axion dark matter: What is it and why now?. Science advances. 2022;8(8)eabj3618. pmc.ncbi.nlm.nih.gov
Gerdy PN. Physiologie médicale, didactique et critique. T. 1. Paris: Librairie de Crochard, 1833. books.google
Maldonado DR, Glein RM, Domb BG. Arthroscopic acetabular labral reconstruction: a review. Journal of hip preservation surgery. 20207(4)611-20. academic.oup.com
Mortensen AJ, Johnson BT, Featherall J, Mills MK, Metz AK, Froerer DL, Aoki SK. Increased Labral Height is Associated with Greater Distractive Stability of the Hip: An In Vivo Analysis. Arthroscopy: The Journal of Arthroscopic & Related Surgery. 27 March 2025. sciencedirect.com
Pauwels F. Biomechanics of the locomotor apparatus: contributions on the functional anatomy of the locomotor apparatus. Berline [etc.], Springer Science & Business Media, 2012. books.google
Ruhmann O, Borner C, von Lewinski G, Bohnsack M. Ligamentum teres. Orthopade. 2006;35(1)59-66. link.springer.com
Strange FGStC. The hip. London: William Heinemann Medical, 1965. amazon.co.uk
Westermann RW, Day MA, Duchman KR, Glass NA, Lynch TS, Rosneck JT. Trends in hip arthroscopic labral repair: an American Board of Orthopaedic Surgery Database Study. Arthroscopy: The Journal of Arthroscopic & Related Surgery. 2019;35(5)1413-9. arthroscopyjournal.org
Архипов СВ(a). Моделирование взаимодействия LCF нормальной длины и отводящей группы мышц. О круглой связке бедра. 09.06.2024. kruglayasvyazka.blogspot.com
Архипов СВ(b). Моделирование взаимодействия удлиненной LCF и отводящей группы мышц. О круглой связке бедра. 09.06.2024. kruglayasvyazka.blogspot.com
Архипов СВ(c). Моделирование взаимодействия LCF нормальной длины и отводящей группы мышц. О круглой связке бедра. 09.06.2024 kruglayasvyazka.blogspot.com
Архипов СВ(d). Моделирование взаимодействия LCF, вертлужной губы и отводящей группы мышц. О круглой связке бедра. 12.06.2024. kruglayasvyazka.blogspot.com
Архипов СВ. Роль связки головки бедренной кости в патогенезе коксартроза: дис. … канд. мед. наук. Москва, 2012. medical-diss.com , kruglayasvyazka.blogspot.com
Архипов СВ. Связка головки бедренной кости: функция и роль в патогенезе коксартроза; 2-ое изд., испр. и доп. Йоэнсуу: Издание Автора, 2023. books.google
Малахова СО. Артроскопия тазобедренного сустава (клинико-экспериментальное исследование): Дисс. … канд. мед. наук. Москва, 2001. cito-priorov.ru
Орлецкий АК, Малахова СО, Морозов АК, Огарев ЕВ. Артроскопическая хирургия тазобедренного сустава. Под ред. акад. С.П. Миронова. Москва, 2004. kingmed.info
Reviews
First reviewer
Grok, Artificial Intelligence, Developed by xAI.
Second reviewer (after revision of the article)
ChatGPT, a language model trained to assist with text analysis and editing OpenAI,
2025.
Address correspondence to Arkhipov Sergey, M.D., E-mail: archipovsv@gmail.com
Cite:
Online version:
Arkhipov
SV. Why Acetabular Labrum
Repair May Be Ineffective: A Note on the Mysterious ‘Dark Matter’ in the Hip
Joint. About round ligament of femur. April 7, 2025. https://roundligament.blogspot.com/2025/04/2025arkhipovsv-why-acetabular-labrum.html
PDF version:
Arkhipov SV. Why
Acetabular Labrum Repair May Be Ineffective: A Note on the Mysterious ‘Dark
Matter’ in the Hip Joint. About round ligament of
femur. April 7, 2025; 1-6. DOI: 10.13140/RG.2.2.26370.59842 ,
© 2025 Arkhipov S.V. This is an open access article under
the CC BY-NC-ND license (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Additions
No.
History of the article:
First publications in the online magazine:
[Ru] Архипов СВ. Почему восстановление вертлужной губы может быть неэффективно?: Заметка о таинственной «темной материи» в тазобедренном суставе. О круглой связке бедра. 06.04.2025. https://kruglayasvyazka.blogspot.com/2025/04/2025.html
PDF version:
[Ru] Архипов СВ. Почему восстановление вертлужной губы может быть неэффективно?: Заметка о таинственной «темной материи» в тазобедренном суставе. О круглой связке бедра. 06.04.2025; 1-7. DOI: 10.13140/RG.2.2.14659.31520 , researchgate.net, Google Drive
[En] Arkhipov
SV. Why Acetabular Labrum Repair May Be Ineffective: A Note on the
Mysterious ‘Dark Matter’ in the Hip Joint. About
round ligament of femur. April 7, 2025; 1-6. DOI: 10.13140/RG.2.2.26370.59842 ,
NB! Fair practice / use: copied for the purposes of criticism, review, comment, research and private study in accordance with Copyright Laws of the US: 17 U.S.C. §107; Copyright Law of the EU: Dir. 2001/29/EC, art.5/3a,d; Copyright Law of the RU: ГК РФ ст.1274/1.1-2,7
Comments
Post a Comment